


Dr. Andrew Robertson presided over mass vaccine injuries during ‘covid zero' then issued mandates.
UN Iraq weapons inspector and bioterrorism expert could have saved countless lives - who gave the orders?


Welcome article for new readers: battlefield philosophy and my articles summarised
Support ExcessDeathsAU with a small one-off donation (Ko-Fi)
ExcessDeathsAU has been banned from social media: I rely on you to share articles
Dear Readers,
When I saw Dr/Mr Anthony Fauci recently take the stand I knew that it was time to publish this article.
You see, all over the world, certain people are elevated to high-ranking medical positions for a reason; they are not there by accident.
Evidence indicates that their real task differs from their ostensible task, and with those for eyes to see, this became particularly clear very early on in 2020 when examining the covid response.
When it becomes evident that senior doctors are hurting people en masse, it is incumbent on their colleagues to blow the whistle, and their superiors to remove them from further ability to harm, accompanied by criminal charges. A key example of failure is when (for example) public health data show that a lot of people start getting sick and/or dying after a novel ‘public intervention.’
However, of course, their superiors have been elevated to these positions for the same reason, and when there are no stopping conditions, such as during an Emergency, there are no levers to pull.
So what do these chief medical officers do? Who are they?
Please meet Dr. Andrew Robertson who is the ‘Chief Health Officer’ of the Australian state of Western Australia (WA). His official title is: Assistant Director General and Chief Health Officer within the Public and Aboriginal Health Division in the WA Department of Health (WA Health). According to the WA Government website, Robertson assumed this position in 2018 and is still currently filling this position as of June 2024.
Like Fauci, Robertson is a bureaucrat.
The ‘covid situation’ in Western Australia was unique, but hugely important to the rest of the world. Catastrophically large rates of vaccine injuries were officially recorded by the West Australian government during ‘covid zero’ for 10 months straight in 2021. No one could have blamed this injury rate (like myocarditis or pericarditis) on ‘covid.’
During months 8-10 of this situation, a high-level vaccine group met in Western Australia that discussed mandating vaccines (which they did), risks, vaccine hesitancy, and jabs for children 5-11 and boosters. Chief Health Officer Andrew Robertson was the highest-ranking health official at these meetings, and according to parliamentary papers he attended every meeting.
This was (and still is) the global smoking gun for vaccine harm.
It is my opinion that Andrew Robertson, acting in his official capacity, given his exceptional expertise and research track record in public health, military strategy, and biowarfare, was perfectly placed to have blown the whistle and saved millions of lives, and perhaps prevented hundreds of millions of men, women, and children around the world from receiving boosters or additional doses of the covid vaccine.
Robertson also has great expertise in other areas of public health that are relevant and helpful to Australians. However, he not only chose not to do any of this, he doubled down, stayed silent, and then mandated the covid vaccine for healthy workers in Western Australia.
In this article I present the evidence, but also query who is really giving the orders.
Thank you for paid subscribers who keep articles free for everyone around the world.
God Bless you readers, wherever you are.
Yours Faithfully,
ExcessDeathsAU
11 When the sentence for a crime is not quickly carried out, people’s hearts are filled with schemes to do wrong.
Ecclesiastes 8:11
Essential background reading



Article Structure
I. Western Australia during ‘covid zero’ - vaccine rolls out and injuries explode.
II. Chief Health Officer Andrew Robertson presides over mass vaccine harm then issues vaccine mandates.
III. Andrew Robertson’s published CV (IIIa.) and select research papers relevant to covid response (IIIb.).
IV. Final thoughts: Who gave the orders?
V. Mistakes Were NOT Made: An Anthem for Justice (Poem by Margaret Anna Alice; Read by Dr. Mike Yeadon).
I. Western Australia during ‘covid zero’ - vaccine rolls out and injuries explode
Like many people around the world, Australians really did not pay much attention to ‘public health officials’ before covid (or if you are like me, during covid). This article written 29 November 2020 “The rise of the Chief Health Officer: How Dr Andy Robertson became a household name” actually captures quite a lot of Australian sentiment at the time. (Archive).
However, it is extremely important for setting the scene of what we are seeing.
At the start of this year, few people knew the identity, or even existence, of their State’s Chief Health Officer (CHO).
Now these quietly-spoken medical officials have been propelled from the relative obscurity in their work behind the scenes into the limelight at a never ending barrage of press conferences.
The life-altering decisions made on the basis of their expertise has arguably made CHOs the most important people in their States.
The phrase “based on the medical advice” has been uttered countless times by premiers and prime ministers as they announce restrictions…
Catherine Bennett, chair of epidemiology at Deakin University, said the CHOs were the “face of the public health response” to COVID-19.
“They work collectively to some degree through the Australian Principal Health Protection Committee. It’s important that there is co-ordination between the States and that they can use each other as sounding boards,” she said.
“At the other end, they are heading up public health teams. They’re kind of that pivotal person in the middle that provides leadership at State level and helps that co-ordination nationally.”
In WA, the CHO is responsible for the State’s public health and advises the Health Minister, and the community generally, on public health matters.
The article then describes health officers around the world in similar roles to Robertson such as: Chris Whitty (UK), Anders Tegnell (Sweden), Anthony Fauci (USA).
Archie Clements, professor of infectious diseases and epidemiology at Curtin University, said the pandemic response had become “heavily politicised” in the US, while in Australia, governments had taken risky political decisions early on based on medical advice.
“I think that our governments been very good at harnessing the available knowledge bank in the country and I think they have listened to the chief medical officers. I think that’s why we’re in such a good position,” he said.
The article then goes back and forth about how much of the decision making is ‘political’ and how much of it is ‘scientific.’ However, what is clear is that when Australian politicians say “based on the health advice” they are referring to their Chief Health Officer. In the case of Western Australia, that is Andrew Robertson.
I have written previously about the cognitive warfare deployed by the West Australian State government (likely via Federal military assets) on the people to create hysteria conditions so will not go into it here. However, ‘maintaining covid zero’ via ‘hard borders’ was a key aspect of the psychological abuse:

Under these ‘covid zero conditions,’ the covid vaccines were initially deployed to the citizens with, again, increasing levels of psychological abuse until it all quickly fell apart (see above article, particularly section VI. Critical public bootcamp timeline – where “legal advice” and “health advice” changed from moment to moment before finally collapsing).
But what I want to focus on is the official government record of vaccine injuries during ‘covid zero.’ The most detailed analysis of this report can be found at
:
In 2021, adverse events following immunisation (AEFIs) with the Covid vaccines were reported at almost 24x the rate (per 100, 000 doses) of AEFIs for all other vaccines combined.

They will try to gaslight you with the y-axis showing ‘count of individual event reports’ but remember that the data show a rate (please open the article and read it). Therefore, they cannot get away with the trope ‘oh - we were vaccinating so many people, that’s why there were so many injuries!”
NO.
And keep remembering, according to the government, there was no (or very little) ‘covid’ in the population. Even to those deep into the official narrative of ‘testing’ and ‘cases’ and ‘spread’, the vaccine deployment in Western Australia in 2021 was intentional mass public harm.
They did not stop because they did not want to.
I also reported on this situation, further emphasising how data was probably a massive underreporting of injuries, given how doctors were being threatened with deregistration if they ‘said anything that was negative, or could be perceived as anti-vaccination.’

The case of WA’s vaccine data even captured the eye of Dr. John Campbell who published a video on it on 13 July 2023. As usual, he nicely breaks down the data for a lay audience (as of June 2024, it has had 501K views):
II. Chief Health Officer Andrew Robertson presides over mass vaccine harm then issues vaccine mandates.
In the below article I wrote:
…in 2021, someone gave the order to keep jabbing, and the employees watching the data remained silent, following the orders to keep jabbing and ignoring the harm data.
The people in the WA Health Department are specialists in health statistics and data. They knew exactly what they were looking at when those numbers popped up on the screen, and when it kept happening month after month, they would have known that it was not an accident.
The WA Vaccination Strategic Coordination Group was announced on August 24, 2021. From the announcement: (Archive)
To support the operational delivery of the vaccine program, the Chief Operating Officer of the Vaccine Program within the Department of Health, along with a small project team comprising relevant experts in data analysis, project management, logistics, communication and engagement will report directly to the Vaccine Commander.1
The WA COVID-19 Vaccine Commander will report directly to the Premier and Health Minister, and a Vaccination Strategic Coordination Group will be established to support the Commander.

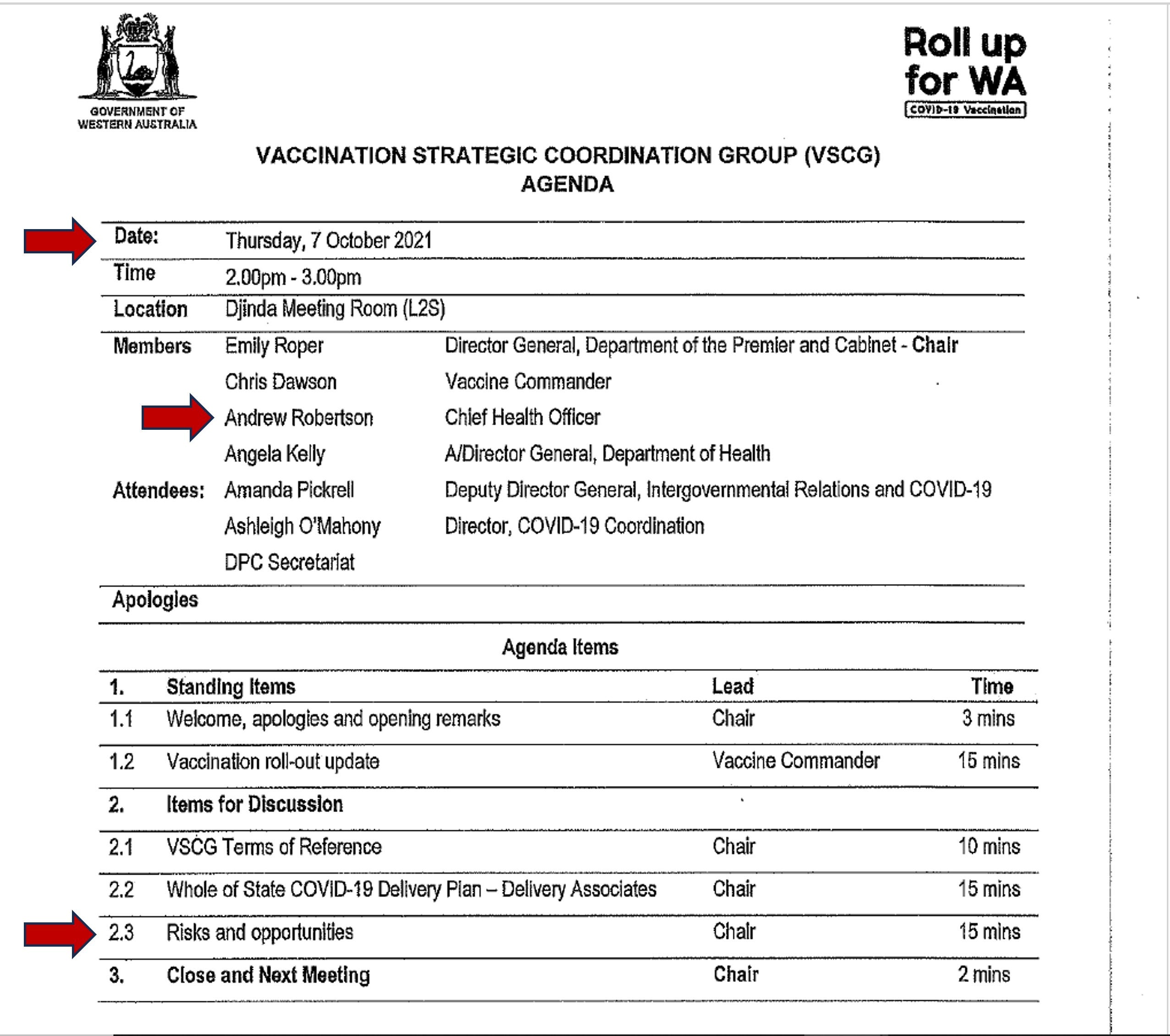
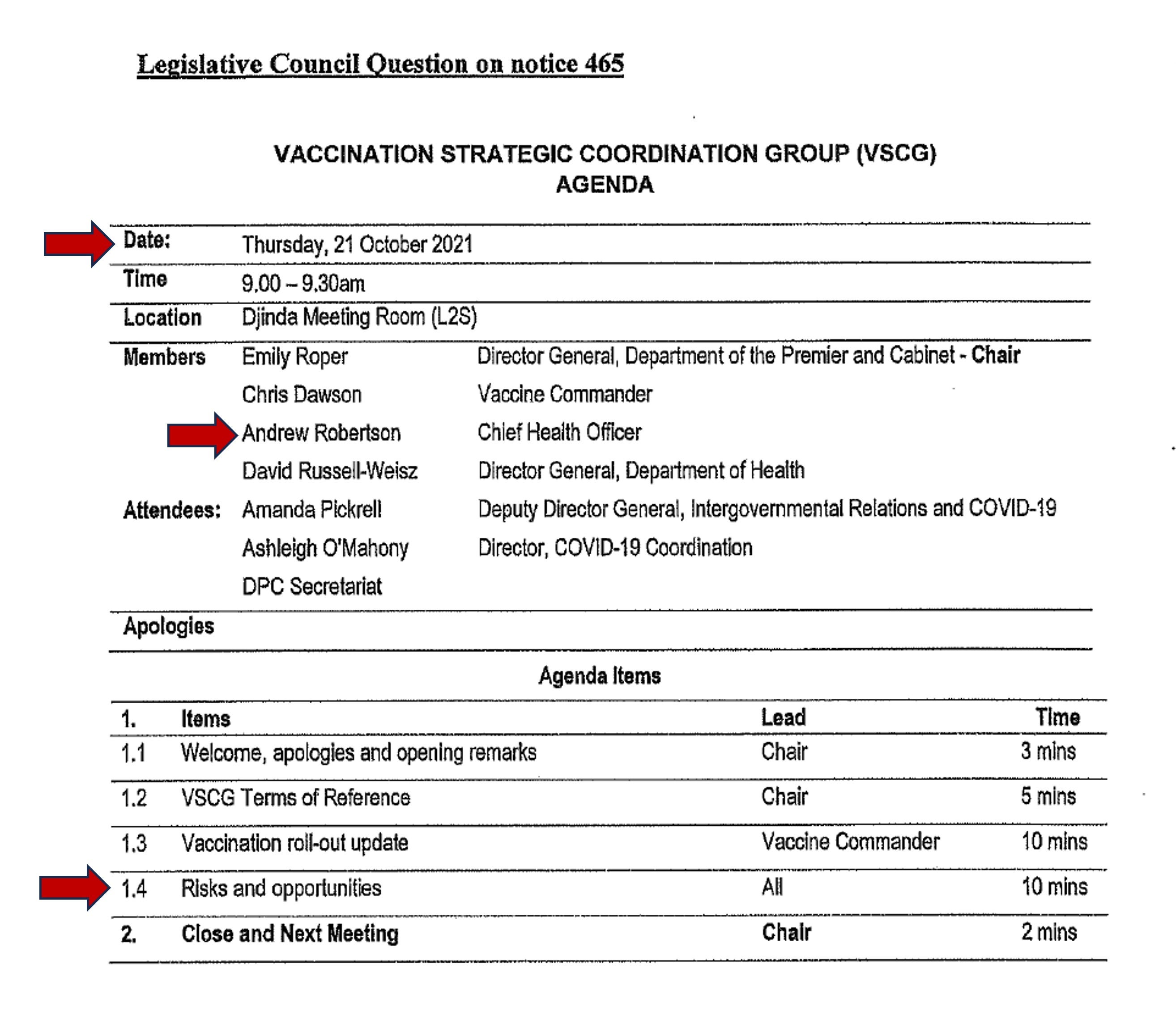
Here are the public papers tabled by WA Parliament showing when the Vaccination Strategic Coordination Group met and who was at each meeting:
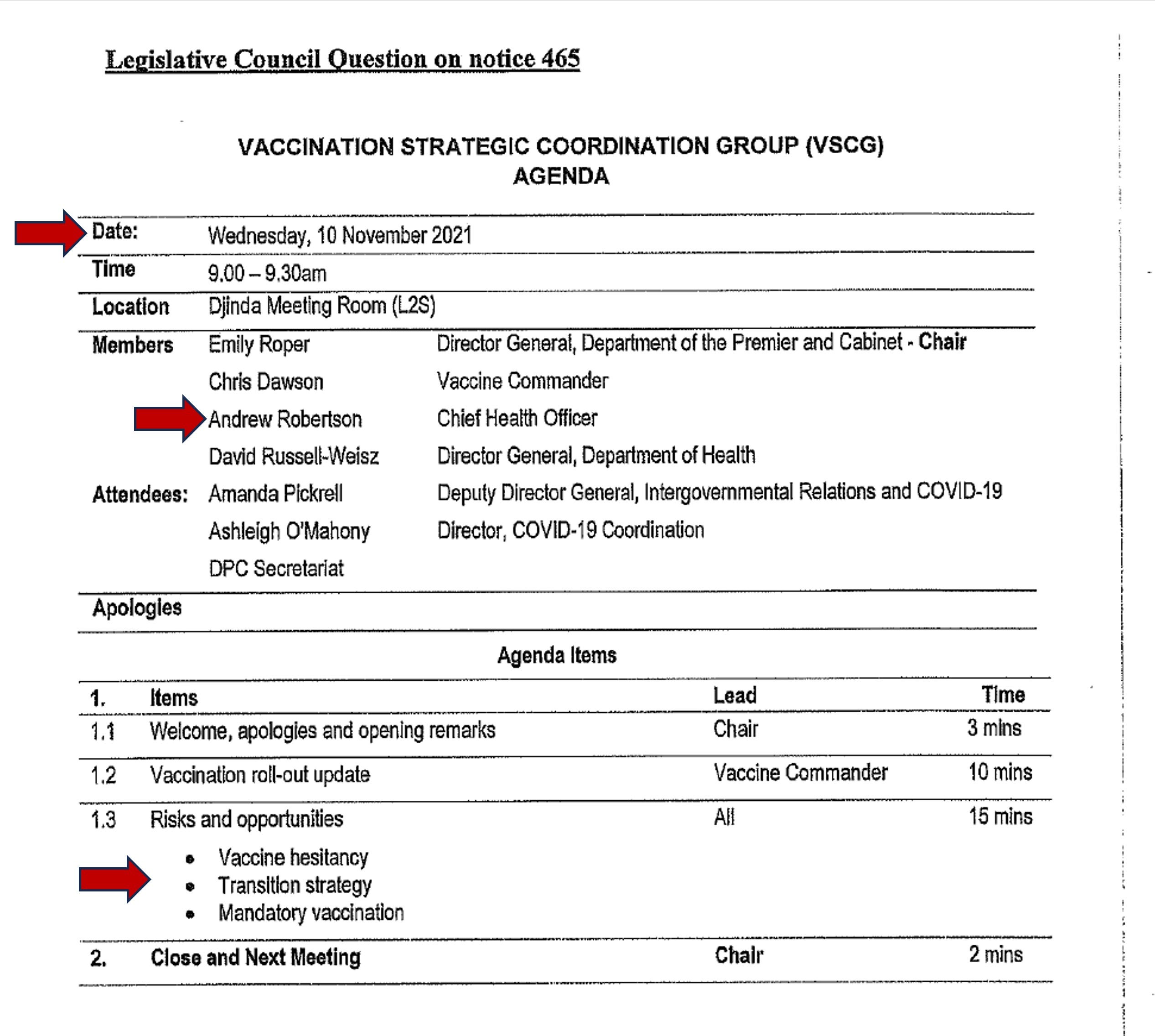
According to this tabled paper CHO Andrew Robertson was at every meeting, and at every meeting there were agenda items about “risks and opportunities” and/or “hesitancy.”
In public health, catastrophic numbers of vaccine injuries (or any deaths) would presumably be considered a “risk” to the rollout of the vaccine, and people experiencing and witnessing real harm to themselves and their loved ones would rightly result in “hesitancy” (i.e., self-preservation instincts).
Even as the catastrophic numbers of jab injuries were officially rolling in, they were discussing boosters and jabbing children 5-11 years old.
***Red arrows on document indicate key words/events: meeting date, Andrew Robertson, risk, booster, children, etc.
Risks and opportunities
Risks and opportunities
Risks and opportunities
Vaccine hesitancy
Transition strategy
Mandatory vaccination
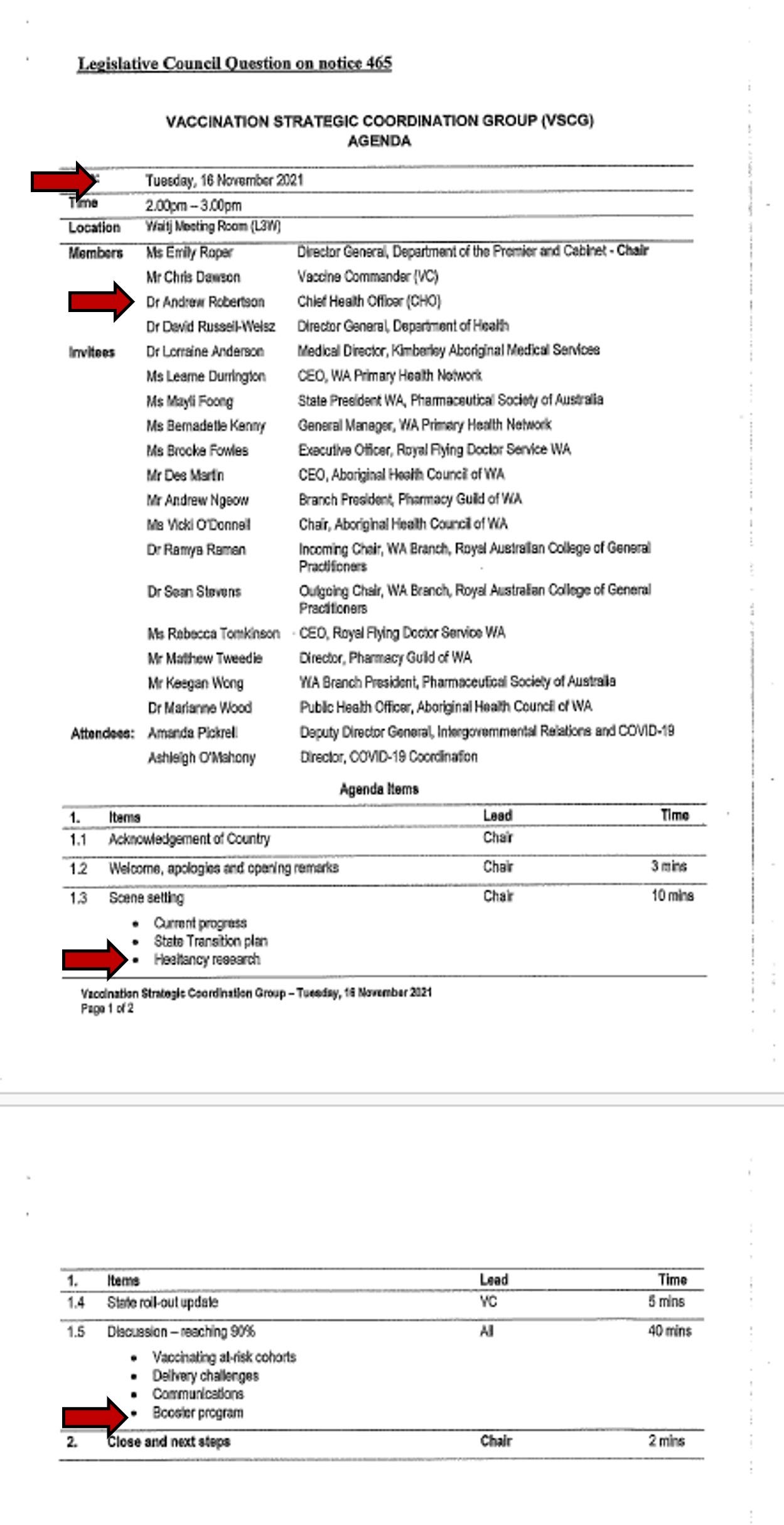
Hesitancy research
Booster program
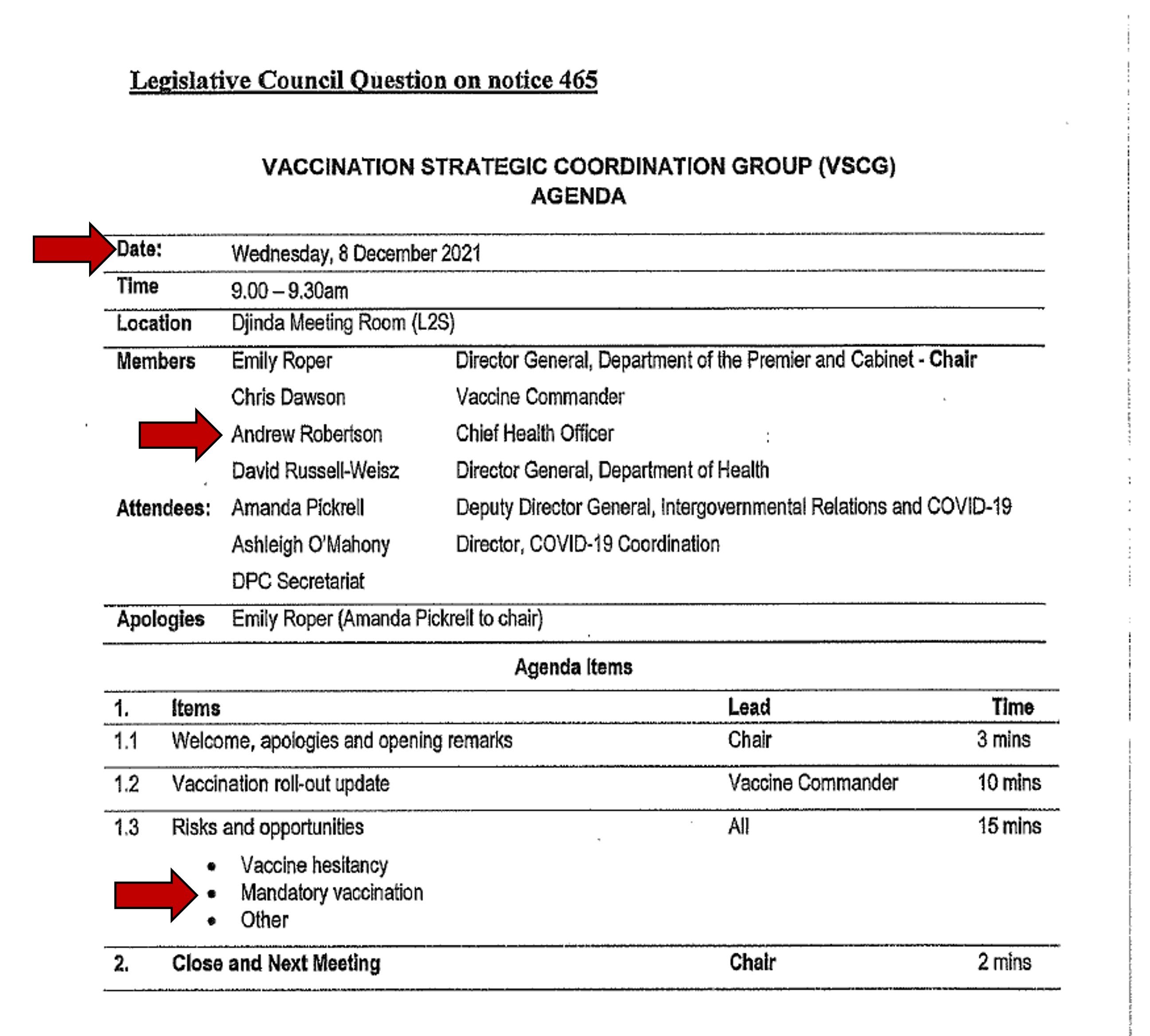
Risks and opportunities
Vaccine hesitancy
Mandatory vaccination
Other
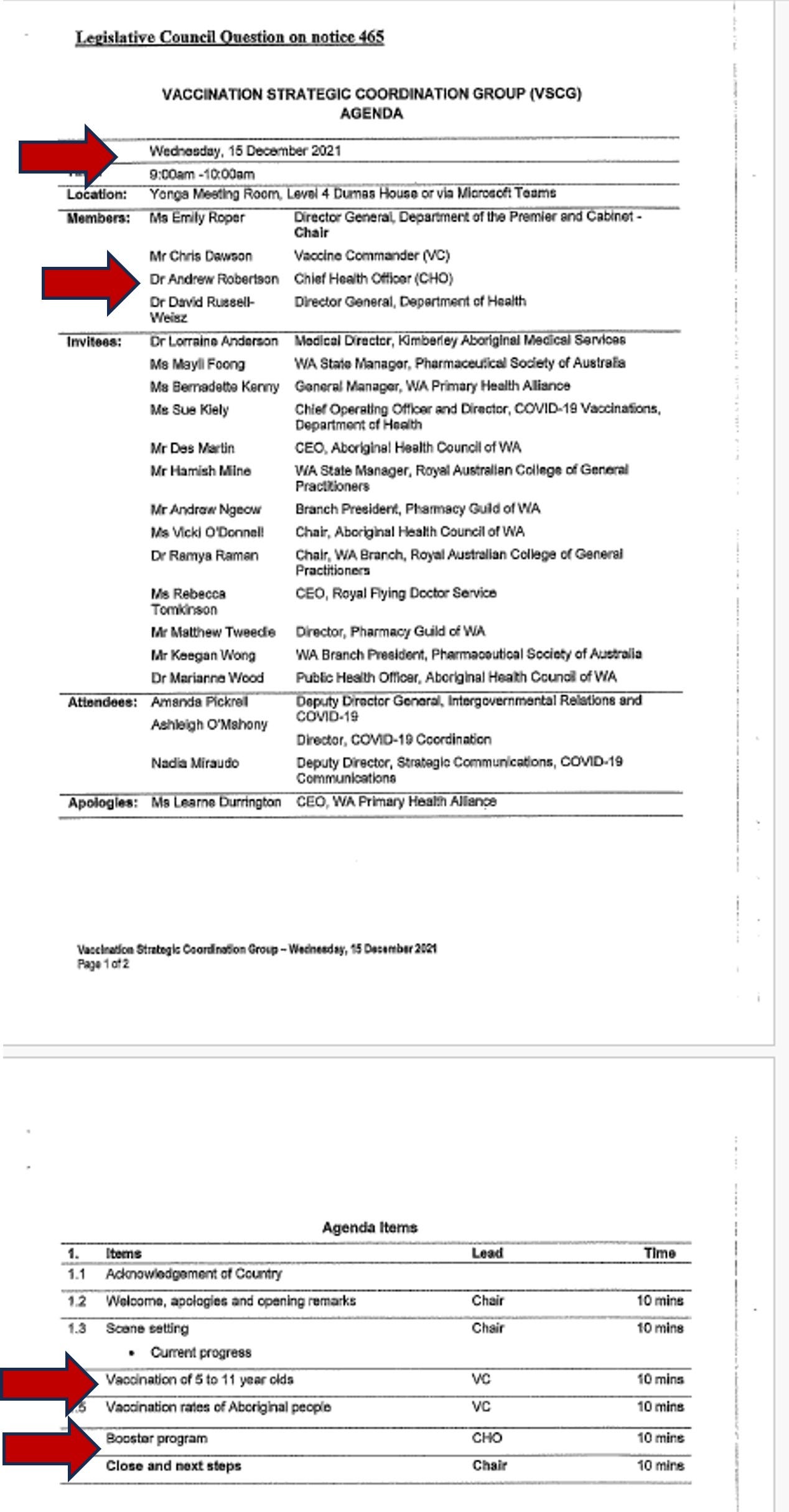
Vaccination of 5 to 11 year olds
Booster program
Then, for emphasis, please see all the Vaccination Strategic Coordination Group meeting dates (one red star - one meeting) as an overlay to the vaccine injury data. Remember, according to the tabled Parliamentary documents Chief Health Officer Andrew Robertson attended every meeting, and again, look how the injuries immediately exploded in March 2021:
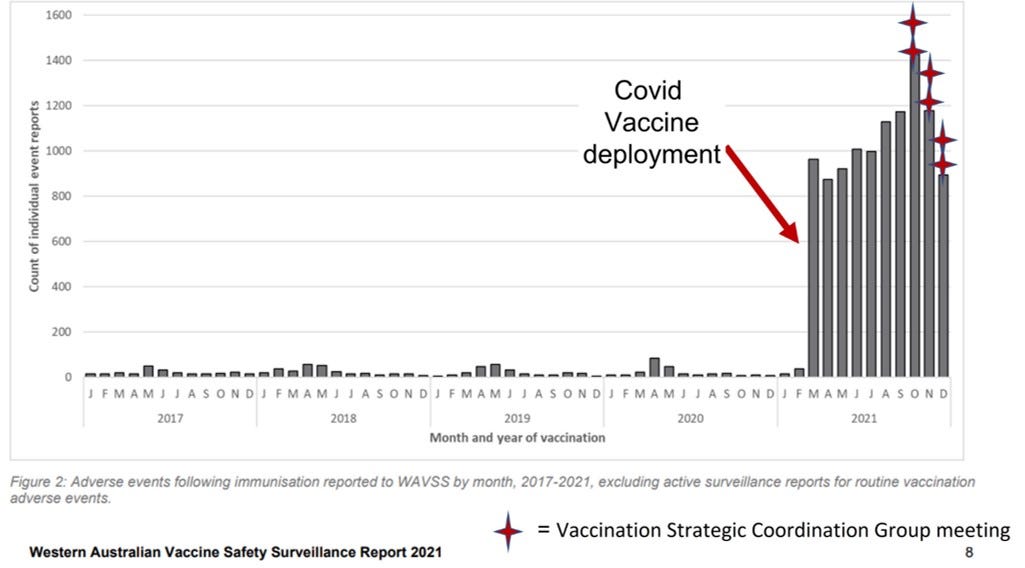
At this point one may wonder: what was happening in the hospitals? All these injured people had to be seen somewhere.

By September 2021 the hospitals in Western Australia were collapsing. (Remember, this was not ‘covid.’ According to the government there was no ‘covid’ in Western Australia. I have to keep emphasising this because people forget).
In Western Australia there were so many hospital presentations that: elective surgery was cancelled, ambulance ramping was at an all-time high, and there were ‘serious hospital workforce shortages.’ (Archive).
What was their response? Vaccinate harder:
More than 1,000 planned surgeries were cancelled across the Perth metropolitan area last month, Parliament has been told, as authorities reveal there has been no modelling to suggest when the state will reach a vaccination rate of 85 per cent.
Health Department director-general David Russell-Weisz said there was significant emergency department pressure and staff sickness in August.
Pressure on the WA hospital system has been at an all-time high in recent months, with a record 6,500 hours of ramping recorded in August.
Mr Cook said utilising the private sector had been a consideration to ease the pressure, but that there was not much capacity to spare.
Meanwhile, the state's top health official said he was yet to see any modelling showing when the state could reach a vaccination rate of 85 per cent.
Chief Health Officer Andrew Robertson told budget estimates the state was on track to hit 70 per cent around mid-November and 80 per cent in the first weeks of December.
Were there any official Australian government data for what happened in Australian hospitals during 2021? Data government health officials could have seen at the time? Yes there were, and the CHOs from all the different states were obliged to meet regularly during the Emergency via the Australian Health Protection Principal Committee. If something was occurring in one state, the others were meant to know.
Please see
elevatingAccording to information released as a result of a freedom of information request (because the public health authorities wouldn’t publish it otherwise) there has been an explosion of serious cardiac episodes in Australia since April 2021.
This public health emergency is disproportionally affecting young people, with emergency department presentations for 10 to 29 year olds almost doubling over the period March 2021 to Feb 2022.
We can safely eliminate COVID as the cause of this very concerning public health emergency since there was absolutely no impact whatsoever when it originally emerged in 2020, and although the second COVID peak coincides with the first peak in increased cardiac episodes, thereafter, as COVID hospitalisations continue to increase, cardiac episodes relatively decrease.

And here come the mandates in ‘covid zero’ Western Australia.
Please see below article from November 2, 2021 where Andrew Robertson personally decides to mandate vaccines, (Archive) all while the above vaccine injuries and hospital collapses and documented harms were occurring during ‘covid zero’:
More than 54,000 doses of Pfizer’s COVID vaccine destined for general practices across WA have been reallocated to the State Government due to unexpected low demand.
The shock figure comes as WA Chief Health Officer Andy Robertson lamented that West Australians weren’t motivated enough to get vaccinated while the State was COVID-free.
In written advice to Mark McGowan dated October 22, Dr Robertson said WA’s slowing voluntary vaccination left him with “little choice” but to mandate the jab for critical workers.
“Despite strong Government messaging regarding vaccination, there is apparently insufficient incentive for WA residents to come forward for vaccination, in the absence of the impetus caused by COVID cases in the community,” he wrote.
The advice added: “With our current low rate of vaccination and a slowing of voluntary vaccination, I am left with little choice but to mandate vaccination in groups that are at risk through their interactions in the community and for those services that will be relied upon should WA experience community transmission and be required to lockdown.”
“It is prudent to strongly message that vaccination is the most effective protective measure, that is available to the community and my intention is that, in the event of a lockdown or major restrictions, it will only be fully vaccinated workers who will be allowed to engage in employment outside the home,” the CHO wrote.
Hi Andy.
Remember us?
December 1, 2021:

III. Andrew Robertson’s published CV and select research papers relevant to covid response.
Below it will be established that Andrew Robertson has the credibility, expertise, access to information and experience to not just understand what he was seeing during ‘covid zero’ in Western Australia with regards to vaccine harms but hospital protocols and other forms of government actions on the people of Australia.
IIIa. Published CV

In addition to his current position as Chief Health Officer of the State of Western Australia, Dr. Andrew Robertson is the Editor-in-Chief of the Journal of Military and Veterans’ Health. (Archive). His full CV may be found on the link provided. Below are key word excerpts - may not be in chronological order:
Deputy Chief Health Officer and Director, Disaster Management from February 2008 until June 2018.
Specialist medical qualifications in Public Health Medicine and Medical Administration, sub-specialty training in Underwater Medicine, Disaster Medicine and Chemical, Biological and Radiological (CBR) Defence.
Royal Australian Navy (1984-2003).
Three tours to Iraq as a Biological Weapons Chief Inspector with the United Nations Special Commission in 1996 and 1997.
Sea-postings on HMAS CANBERRA, HMAS SYDNEY and HMAS PARRAMATTA.
Director Naval Health Reserves – WA from December 2006 to July 2015.
Provided specialist medical advice as an advisor to the Sea Worthiness Boards.
Deployed as a public health specialist on Pacific Partnership in 2015 and 2016.
Pacific Partnership is an annual deployment of forces from the Pacific Fleet of the United States Navy in cooperation with regional governments and military forces, along with humanitarian and non-government organizations.

July 2015. Promoted to Commodore and undertook the role of Director General Navy Health Reserves until December 2019.
October 2003. Director, Disaster Preparedness and Management in WA Health.
December 2004. Led the Australian Medical Relief team into the Maldives post tsunami.
2005. Managed WA Health’s response to the ‘Bali Bombing II.’
June 2006. Led the WA Health team into Indonesia after the Yogyakarta earthquakes.
2011. Radiation Health Adviser to the Australian Embassy after the Fukushima nuclear incident.
2015. Conducted the AUSMAT needs assessment in Nepal after the Nepal earthquake.
Since 2008, he has coordinated the WA Health responses and acted as the Chief Information Officer and the Chief Medical Officer to:
Cyclone George
Varanus Island gas explosion
Ashmore Reef incident
2009 H1N1 pandemic
2011 CHOGM meeting
2015 Ebola preparations
(Robertson) has been undertaking his current role since June 2018, including leading the WA Health response to the Coronavirus Disease 2019 (COVID-19) outbreak.
IIIb. Select research papers relevant to covid response.
Readers please note, papers are not in any particular order and the below list is not comprehensive. Andrew Robertson’s full list of publications may be found at Google Scholar.
From Asps to Allegations: Biological Warfare in History. Military Medicine. 1995.
Biological warfare has been waged intermittently for nearly 2,500 years. The techniques of delivery and weaponization of biological warfare agents have gradually evolved from the catapulting of plague victims to the deliberate use of infected clothes, insect vectors, and specialized weapon systems.
Bioterrorism - an Australian perspective. ADF Health. 2000.
Biological warfare agents have been developed in several national military programs.
There are many definitions of terrorism. One of the more succinct defines terrorism as “politically or religiously motivated acts of violence causing non-combatant casualties.
Potential biological warfare agents can be acquired from natural reservoirs, stolen from medical or research facilities, bought from legitimate or “black market” suppliers, or procured from a “friendly” government.
American industry employs around 60 000 biologists and there are nearly 1900 biotechnology companies in the United States and Europe. This expertise, coupled with that available from scientists from past biological weapons programs, gives terrorist groups a plethora of capable people.
There are many means of delivering biological weapons. They could include dispersal of the biological agent as a vapour or aerosol, contamination of food or drink, direct contact (by injection or inoculation)…
A smaller scale attack confined to an enclosed area, including buildings with air-conditioning systems, domed sports stadiums and subway systems, is more feasible.

Vaccine development: the biological weapon imperative. Developments in Biologicals. 2002.
Fulminant liver failure and transplantation after use of dietary supplements. The Medical Journal of Australia. 2016.
In the absence of any alternative cause of hepatotoxicity, an adverse event notification was made to the Therapeutic Goods Administration, detailing the use of the two dietary supplements.
Response to a pandemic (H1N1) 2009 influenza in Australia - lessons from a State health department perspective. Australian Health Review. 2010.
social distancing to avoid transmission
WA began selective partial or full school closures in early June…Evaluation of the school closure program has shown that it was only partially effective in reducing opportunities for transmission, with many children continuing to mix outside of school, and that it produced substantial adverse effects on families, schools and the workforce.
Diagnostic testing was now recommended only for those who were severely ill…
Key questions that needed to be resolved included: the safety and efficacy of the vaccine, particularly when it was initially proposed to release the vaccine before registration
…providers were concerned about indemnity if the vaccine was not fully registered.
Over 1000 WA vaccine providers were trained specifically for the vaccine rollout, given the challenge of using multidose vials.
Mortality data for WA, both in terms of overall deaths and deaths from pneumonia or specific to influenza, supports the proposition that the mortality impact overall of pH1N1 was no greater than that observed in recent years from seasonal influenza…
Lessons learnt will help shape our response in 2010 and beyond.
Regarding the “providers,” please see FOI 2342 published in ExcessDeathsAU article “2020-2022: Australia’s covid response” (below):
FOI 2342 – Letters (x2) from Minister Greg Hunt to RACGP and AMA about covid vaccines.
April 2021
Letter 1 from Minister Greg Hunt to Dr Karen Price (RACGP) regarding vaccine indemnity arrangements, doctor concerns, informed consent, insurance, increased risk of thrombosis with AstraZeneca, ‘updated consent forms,’ ‘maintaining public confidence in the rollout,’ government contact is Paul McBride.
Letter 2 from Minister Greg Hunt to Dr Omar Khorshid (AMA), contents much as above.

Adolescent psychologist Michael Carr-Gregg said school closures, service disruptions and remote learning not only stunted the educational progress of young people, but increased their stress, isolated them and reduced their physical activity.
Chief executive officer of Catholic Schools NSW Dallas McInerney said for many key decisions, including those made in emergency cabinet meetings, “there was no schools’ voice in the room”.
“So who gave the advice, and who had the ear of the government, was the public health officials. I think whatever legacy or maladies of the school closures, the public health officials own that, and those who accepted their advice,” McInerney said.

Pre-and post-deployment health support provided to Australian Disaster Medical Assistance Team members: Results of a national survey. Travel medicine and Infectious Disease. 2009.
Following the return home, and in addition to mission and psychological debriefing, there should be a post-deployment medical examination and ongoing support and follow-up of DMAT members. More research is needed to examine deployment health support issues.
Many health care professionals around Australia spoke out about what they were seeing in hospitals in terms of vaccine and hospital protocol injuries to themselves and others and were fired, censored, debanked, imprisoned, thrown out of society, deregistered, bankrupted, and divorced.

The health consequences of economic crises. Emerging Threats Journal. 2009.


The medical effects of non-lethal weapons - a review. Australian Military Medicine. 2005.
Natural disasters and the lung. Respirology. 2011.

This article (Natural disasters and the lung) references ‘lessons learned’ from Hurricane Katrina in 2005 twice.
Now we remember what happened to people’s ‘lungs’ at Memorial Hospital in New Orleans according to their hospital protocols.
Andrew Robertson is an expert in disasters and Hurricane Katrina is one of the most important humanitarian disasters in modern times. Strangely, this was not in Dr Robertson’s article. This was not one of the ‘lessons.’

The deadly choices at Memorial. (Archive - The New York Times Magazine).
During Hurricane Katrina in 2005, Americans at Memorial Hospital that were ‘not even near death’ were euthanised using midazolam and left to die in the basement of a flooded hospital in New Orleans during a government State of Emergency.
…it appears that at least 17 patients were injected with morphine or the sedative midazolam, or both, after a long-awaited rescue effort was at last emptying the hospital. A number of these patients were extremely ill and might not have survived the evacuation. Several were almost certainly not near death when they were injected, according to medical professionals who treated them at Memorial and an internist’s review of their charts and autopsies that was commissioned by investigators but never made public.
The physician, Anna Pou, defended herself on national television, saying her role was to “help” patients “through their pain,” a position she maintains today. After a New Orleans grand jury declined to indict her on second-degree murder charges, the case faded from view.
In the four years since Katrina, Pou has helped write and pass three laws in Louisiana that offer immunity to health care professionals from most civil lawsuits — though not in cases of willful misconduct — for their work in future disasters, from hurricanes to terrorist attacks to pandemic influenza.
IV. Final thoughts: Who gave the orders?
It is incomprehensible that someone as credentialed as Andrew Robertson, a chief health and information officer, did not understand what he was seeing, did not understand the design and impact of the vaccines, did not understand the military nature of the covid response, did not understand how many people were suffering, did not understand that health care worders were blowing the whistle, did not understand that Australians were sick and dying from the government’s actions, did not understand the effects of the hospital protocol, or that he ‘could not have predicted’ what would happen.
It is incomprehensible that someone as credentialed as Andrew Robertson did not understand the concepts of natural immunity and relative vs. absolute risk, or was incapable of searching the literature for treatment protocols or indeed remembering his own research. It is incomprehensible that an expert in biowarfare did not understand that a thin cloth over the face of a small child was a compliance and whole-of-society cognitive warfare device.
However, ‘Andrew Robertson’ is not unique. These ‘medical officers’ are now in every town, in every hospital, in every county, in every city, in every country in the world. What is unique about Robertson is that he had real time access to unique government data in Western Australia that could have shut down the vaccine roll out to the entire world.
The ‘covid vaccine’ is not safe and effective. None of them are. They are bioweapons designed to maim, render infertile and kill through multiple vectors inherent in their design.
***Edit: Update July 6, 2024: Please see Dr Francis Boyle, bioweapons expert with experience in human rights, war crimes and genocide, nuclear policy and bio-warfare and architect of the 1989 Treaty Against Bioweapons detail how the ‘covid vaccines’ are biological weapons: interview here with
“MRNA COVID Vaccines Are Bioweapons.”Dr. Boyle’s affadavit published here by

What many of us have painfully learned these past few years is that when an Emergency is declared there is no stopping condition. There is only the Emergency. At that point your life is in your own hands. No one is coming to save you – not your local police, not the judge, not the local council, not the Governor General, nobody.
And definitely not your Chief Health Officer.
The only thing you have is you, your faith, your courage, and if you are very lucky, a few good family members and neighbours.
However, what has been difficult throughout the Emergency in Australia is determining exactly who was in charge, and who was giving the orders.
I mean really giving the orders.
Andrew Robertson has taken responsibility for issuing the mandates after presiding over the vaccine harm data and has specifically told the media (he is) “not being muzzled or hidden away by anybody” (Archive). Therefore, by his own account, he could have spoken out at any time.
The covid response in Australia was a joint domestic military operation with the US Department of Defence, all the way from the first ‘pandemic modelling’ with DTRA on 3 February 2020, to vaccine creation under Operation Warp Speed, and the shared US-Australian expertise of the Generals in charge of Australia’s covid response:
In the US, investigative researcher
has determined that “Fauci Was NOT in Charge of Covid Policy. The National Security Council Was” but still asks the question: Who was actually in charge, and why?
On July 10, 2021, The Guardian attempted to determine the chain-of-command for the military covid operation in Australia (Archive). During the course of their investigations they were hit with stonewalling, confusion, and obfuscations from the government, in particular: “(t)here was concern over the “tone” of the article, or why it was being written.” Although General Frewen stated that he reported to the Prime Minister (Scott Morrison), there was rather a lot of finger-pointing about who was really in charge.
Dear readers, this is how democide and genocide is conducted. When ‘no one is in charge,’ no one is responsible. When people are thrust in the spotlight as the ones ‘taking responsibility,’ they are the ones who will take the fall – politicians and bureaucrats are the veneer for the military-industrial complex, who are the enforcers for the banks, who pull the levers for the real owners, who prostrate to the Monster. That is why it is up to men and women of good conscience to say no, to understand that no one is coming to save them.
Remember what happened during Nuremberg, how the middle management swung and the architects went on to glory under Operation Paperclip or the comfort of obscurity. Even if the killing was legal under the covid Emergency, it continually amazes me that the forward-facing people in the covid response do not consider this.
They always believe they are able to escape their own history.
V. Mistakes Were NOT Made: An Anthem for Justice (Poem by Margaret Anna Alice; Read by Dr. Mike Yeadon).
Credit to
and
The ‘Vaccine Commander’ is former Police Commissioner Chris Dawson - shown in the police uniform - cover photo between Robertson and McGowan. He has been rewarded for his services as Vaccine Commander by an appointment to Governor of Western Australia - the King’s representative to the state. He now lives in a beautiful mansion at the taxpayer’s expense: https://archive.li/0peJI
Dear Readers,
Thanks to your efforts, as of June 12 this article has now been seen 4k times (an increase of 500 from when I sent out the email).
However, I looked at my dashboard and saw the following:
2% social media views.
This means that sharing this on social media is useless - no one is seeing it due to shadowbanning. Re-Stacking this is futile - we are in an echo chamber - people do not even know that Substack exists, and we are siloed within Substack.
So, if you are motivated, please:
-email this to one friend, and one person in the media/government.
If you are not interested, that’s ok. Thanks for reading.
And please see:
Quantitative evaluation of whether the Nobel-Prize-winning COVID-19 vaccine actually saved millions of lives By Denis G. Rancourt, PhD, and Joseph Hickey, PhD.
https://denisrancourt.substack.com/p/quantitative-evaluation-of-whether
Abstract
Fantastic statements that the Nobel-Prize-winning COVID-19 vaccines saved millions (and tens of millions) of lives are based on the theoretical scenarios of Watson et al. (2022), published in The Lancet Infectious Diseases. Watson et al. (2022) theoretically inferred massive mortality reductions distributed globally, occurring solely during vaccine rollouts. We calculated the quantitative consequences of Watson et al. (2022)’s low-value (14.4 million lives saved) theoretical scenario on all-cause mortality by time (by week or by month, 2020-2022) in 95 countries. Our calculations provide graphical proof that the theoretical proposals of Watson et al. (2022) are untenable, compared to measured all-cause mortality. Therefore, the characteristics of the COVID‑19 vaccines (efficacies in preventing infection or serious illness, duration of protection, waning, etc.) and of COVID-19 spread input by Watson et al. (2022) must be invalid.